HAE is a rare and potentially life‑threatening condition1-3
Don’t miss what’s next in HAE
HAE causes recurrent attacks of angioedema ranging from disabling peripheral swelling and painful abdominal episodes to potentially life-threatening laryngeal edema4
HAE has three recognized types
HAE TYPE 1
Low C1INH
levels
People have low levels of C1 inhibitor (this is the most common type, affecting about 85% of cases)5
HAE TYPE 2
C1INH does not
function properly
People have adequate levels of C1 inhibitor, but the protein does not function properly5
HAE WITH
NORMAL C1 INHIBITOR (C1INH)
Normal C1INH
levels and function
A more rare type where people have normal levels and function of C1 inhibitor and can occur with or without an identifiable genetic mutation5
HAE attacks can be unpredictable, Disfiguring, and debilitating imposing a significant burden on people’s lives1,8,9
The unpredictability of attacks can cause anxiety over when the next attack might occur, its severity and location, and the extent of management required.1,9
During an attack, people with HAE may experience many complications
face
- Facial angioedema can impair vision due to periorbital swelling and eyelid closure9,10
- The prominent nature of facial swelling can provoke unwanted attention and psychological distress9,10
- Facial involvement is highly visible and may lead to social withdrawal9,10
throat
- Shortness of breath3,9-11
- Dysphonia3,9-11
- Choking and fear of death from asphyxiation3,9-11
- Fear of airway compromise associated with the highest emotional burden3,9-11
- Airway involvement necessitates prompt emergency care3,9-11
hands & arms
- Functional impairment during attacks can hinder daily activities requiring hand use and may result in complete inability to use the affected limb3,9,11,12
- Could make it difficult to administer on-demand treatment3,9,11,12
- Patients report that hand swelling can attract unwanted attention in social settings3,9,11,12
abdomen & gi tract
- Mild to severe abdominal pain, nausea, vomiting, and/or diarrhea, which can be mistaken for other causes of abdominal pain, such as appendicitis and small bowel obstruction1,9,10,13,14
- Pain from abdominal attacks commonly restricts physical movement and activity1,9,10,13,14
- Abdominal attacks are often described as debilitating and disrupt daily functioning1,9,10,13,14
- Abdominal involvement is associated with considerable emotional burden1,9,10,13,14
genitals
- Potential for increased frequency of attacks during menstruation, ovulation, and pregnancy4
- Inability to take estrogen-containing oral contraceptives4
- Potential for attacks during childbirth4
legs & feet
- Lower extremity angioedema can impair ambulation3,11,12
- Inability to fit into regular shoes may require adaptive footwear or modified activity3,11,12
With never knowing when, where, why, and how HAE will present itself, there comes naturally a lot of anxiety.15
— Jamie, real person living with HAE

Swelling in HAE is generally a result of EXCESS BRADYKININ PRODUCTION
Bradykinin is a peptide mediator that plays a central role in increasing vascular permeability. In the most common types of HAE, it is generally produced through the kallikrein-kinin system when plasma kallikrein cleaves high-molecular-weight kininogen (HMWK).3,16

Most people with HAE often have an underlying deficiency of functional C1INH that leads to dysregulated plasma kallikrein activity1


In most people with HAE, there is either a quantitative or a functional deficiency of C1INH (as seen in HAE types 1 and 2, respectively).6,16
The loss of C1INH control allows dysregulated activation of plasma kallikrein, resulting in an overproduction of bradykinin.15
Low
C1INH
Uncontrolled
kallikrein
activity
Overproduction
of bradykinin

Activation of bradykinin B2 receptors leads to opening of endothelial junctions, causing vasodilation and increased vascular permeability, with the resultant fluid extravasation into surrounding tissues being the clinical hallmark of HAE17,18

Unlike histaminergic angioedema, HAE does not respond to antihistamines, corticosteroids, or epinephrine.3,15
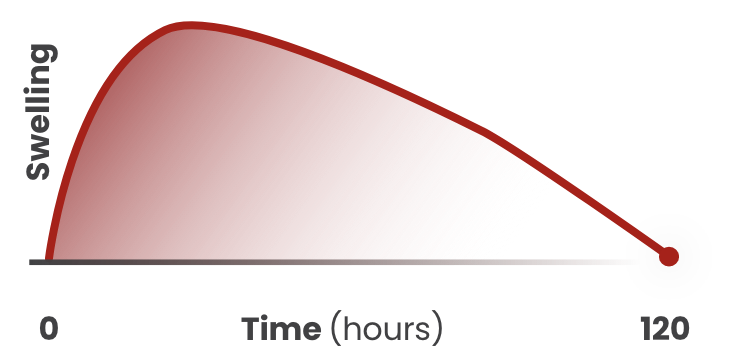
HAE attacks may last for days if not treated
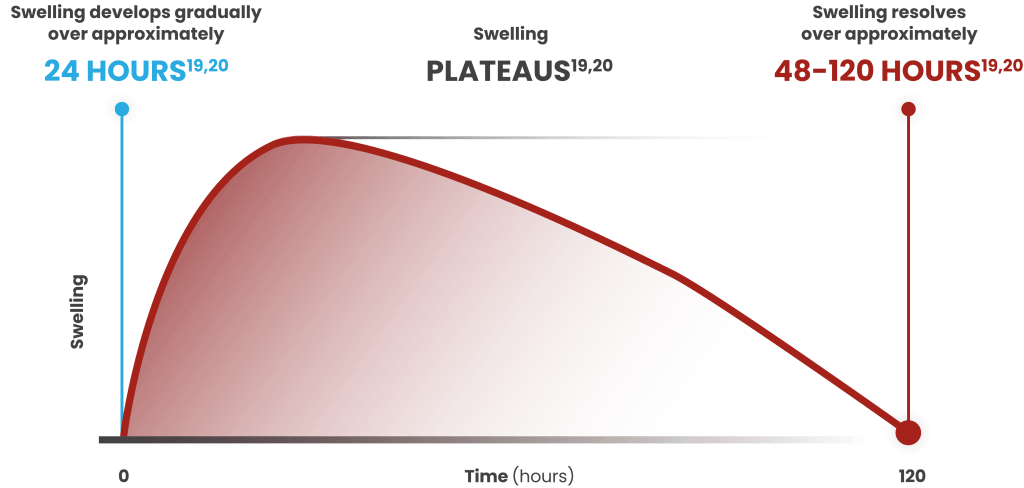
Tap the chart to learn more
Swelling develops gradually
over approximately
Swelling develops gradually
over approximately
Swelling resolves over
approximately
24 HOURS19, 20
PLATEAUS19, 20
48-120 HOURS19, 20
GET THE FACTS
HAE is generally inherited in an autosomal-dominant pattern; the pathogenic mutation is distributed equally among men and women21
Women are sometimes more severely affected than men, as the hormonal effects of estrogen may influence disease activity21
HAE attacks exclusively affecting the face were generally associated with higher absenteeism (26.5%) and work productivity loss (48.2%) than attacks affecting other locations22
In a 2017 survey of 445 people with HAE in the United States:
- 35.3% and 20.9% reported anxiety and depression, respectively22

Burden of HAE Management

Living with HAE
References
- Lumry WR, et al. Allergy Asthma Proc. 2020;41(Suppl 1):S08-S13.
- Christiansen SC, et al. Ann Allergy Asthma Immunol. 2023;131(6):766-774.
- Maurer M, et al. Allergy. 2022;77(7):1961-1990.
- Betschel SD, et al. J Allergy Clin Immunol Pract. 2023;11(8):2315-2325.
- Sinnathamby ES, et al. Adv Ther. 2023;40:814-827.
- Zuraw BL. World Allergy Organ J. 2010;3(9 Suppl):S25-S28.
- Otani IM, et al. Immunol Allergy Clin North Am. 2017;37(3):497-511.
- Anderson J, et al. Allergy Asthma Clin Immunol. 2021;17(1):60.
- Lo SH, et al. Pharmacoecon Open. 2022;6(2):231-239.
- National Organization for Rare Disorders. Hereditary angioedema. Accessed May 22, 2025. https://rarediseases.org/rare-diseases/hereditary-angioedema/
- Food and Drug Administration. The voice of the patient – Hereditary angioedema. Published May 2018. Accessed May 22, 2025. https://www.fda.gov/files/about%20fda/published/The-Voice-of-the-Patient—Hereditary-Angioedema.pdf
- Longhurst HJ, et al. Br J Hosp Med (Lond). 2019;80(7):391-398.
- Gülbahar O. Balkan Med J. 2021;38(2):73-81.
- Zanichelli A, et al. Ann Allergy Asthma Immunol. 2016;117(4):394-398.
- Data on file, Pharvaris.
- Lima H, et al. Front Allergy. 2023;10(4):1-5.
- Busse PJ, et al. N Engl J Med. 2020;382:1136-1148.
- Smith TD, et al. Ann Allergy Asthma Immunol. 2024;133:380-390.
- Manning ME. Allergy Asthma Proc. 2020;41(Suppl 1):S22-S25.
- Bernstein JA, et al. Int J Emerg Med. 2017;10(1):15.
- Hsu E, et al. Allergy Asthma Clin Immunol. 2022;18(64):1-9.
- Banerji A, et al. Ann Allergy Asthma Immunol. 2020;124(6):600-607.


